Story
 November 6, 2014
November 6, 2014
India: Doing the Right Things


The story of 1,000 days–the vital period from the beginning of a woman's pregnancy to her child's...







Minutes after giving birth in the Shivgarh district community hospital in India, new mothers walk down a dark hallway to the maternity ward, a small room crowded with four narrow metal-frame beds. Stained sheets cover the thin plastic mattresses. In this grim setting, a colorful poster taped to the wall features a beaming mom snuggling her baby, along with the message, "In the first hour, a mother can change the fate of her child."
Simple drawings illustrate basic steps that will give the babies a healthy start in life. Sushma, one of the new mothers, recognizes these practices from the women in her village, Rampur Khas. Whenever they meet, on the verandas of their homes or in the fields where they work, the women remind one another of what they can do differently so fewer of their children will die.
Sushma prepared for delivery by buying a new razor blade to cut the umbilical cord, preventing infection, and cotton clothes to keep her baby warm, lowering the risk of hypothermia. Minutes after giving birth, she held her son and began breastfeeding with her antibody-rich colostrum, or first milk. "I know I am doing all I can," she tells me at her home. "I know what I do can make a difference."
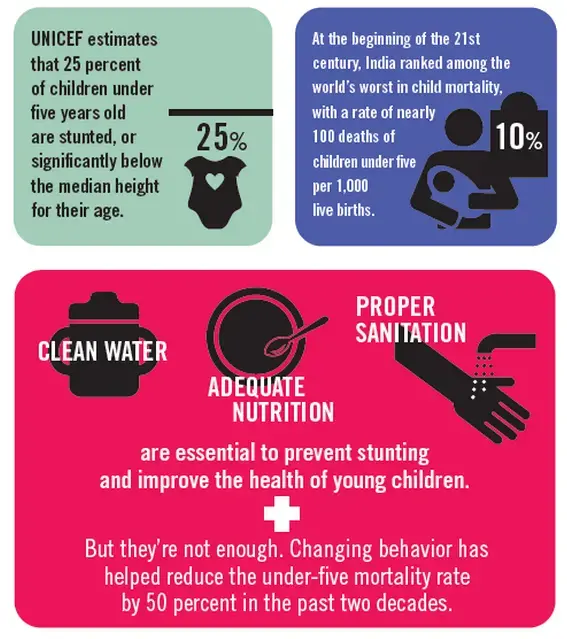
For decades, efforts to improve the lives of children started with getting them into primary school. But the frontline emphasis is shifting to the 1,000 days from the beginning of a woman's pregnancy to her child's second birthday. This is the most critical period in determining lifelong health, when vital micronutrients fuel cognitive and physical development. Stunting that begins in these first 1,000 days can have an irreversible, long-term impact on the ability to learn and work. UNICEF estimates that 25 percent of children under five years old are stunted, or significantly below the median height for their age.
Clean water, adequate nutrition, and proper sanitation are essential to prevent stunting and improve the health of young children. And, in my reporting around the world, I've seen that changing the behavior of expectant and new mothers like Sushma is equally important. Worldwide, this approach has helped reduce the under-five mortality rate by nearly 50 percent in the past two decades.
I see the effects everywhere I travel. In Guatemala, women no longer eat last at every meal, as tradition dictated. In Uganda, expectant mothers now routinely go to a clinic or hospital for prenatal checkups and delivery. In Chicago, they are trading junk food for fresh fruits and vegetables.
Behaviorial change is particularly important in India, which, as a nation, doesn't lack for resources. India was the star of the Green Revolution in the 1960s, when new strains of wheat and rice turned a country plagued by repeated famines into a surplus food producer and emerging agricultural powerhouse. Schools closed during the harvest season so classrooms could store extra grain.
Yet at the beginning of the 21st century, India – for all its advances in agricultural production and high-tech industry – ranked among the world's worst in child mortality, with a rate of nearly 100 deaths of children under five per 1,000 live births. Nearly half of the rest were malnourished and stunted. "The problem of malnutrition is a national shame," former Prime Minister Manmohan Singh has said. "The health of the economy and society lies in the health of this generation."
India passed legislation to fight hunger and began subsidizing food distribution, but these actions alone did little to improve child survival and health. Rather, some of the most effective interventions are proving to be the simplest and cheapest: teaching expectant and new mothers how to care for themselves and their babies.
The Community Empowerment Lab, founded by Vishwajeet Kumar, a doctor who specialized in neonatal and infant health at Johns Hopkins University in Baltimore, helped teach the women in Sushma's village. The group, known by villagers as Saksham, the Hindi word for empowerment, is based in the Indian state of Uttar Pradesh, where child death rates are among the highest in the nation.
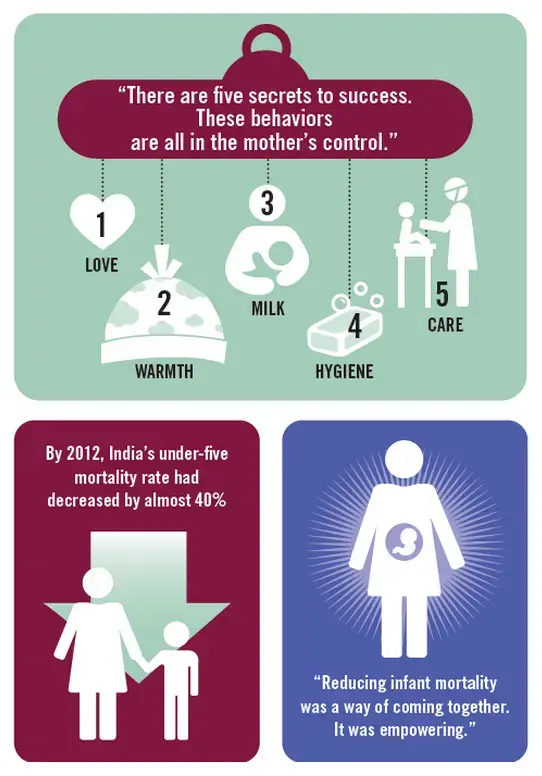
Kumar holds up his right hand and spreads his fingers wide. "There are five secrets to success," he tells me. "One, love. Two, warmth. Three, food – breast milk. Four, hygiene. Five, care – know the signs when the baby is sick and go to the doctor. These behaviors are all in the mother's control."
When Kumar began working in Shivgarh in 2003, nearly all the children appeared stunted. He encountered traditional practices and superstitions that had a devastating impact on newborns. The majority of women delivered their babies at home in unsanitary conditions, scrubbed the infants, and then left them on their own for up to an hour, sometimes more. The ritual was believed to ward off evil spirits, but it also exposed the babies to hypothermia. Breastfeeding didn't begin for several hours at the earliest, or several days in some instances – a mother's first milk was considered unclean and discarded.
"Most of the infant deaths were preventable," he says. "But the communities didn't think change was necessary. They thought the deaths were fated. We had to break this chain of fatalism."
So Kumar established Saksham, and he and his team of community health workers went to the caregivers in the villages – the mothers, the mothers-in-law, the midwives, the spiritual leaders – and demonstrated how some changes in behavior, such as using clean tools, swaddling, and breastfeeding immediately, could increase survival rates. The main message: These are things you can control to improve the health of your newborns. Your children don't have to die.
When the workers encountered resistance to change, they explained the benefits again and again. Sushma's older relatives, particularly her mother-in-law, were skeptical, Sushma says. "But after discussing the changes one, two, three, four times, she accepted. She could see that the babies were healthy, that the mothers were healthy."
Word of mouth carried the message from village to village, to thousands of pregnant women. Songs proliferated. "Hold your child to your breast. Your child will gain weight, get warmth, grow healthy," sang the women of Rampur Khas. In the village of Bharjor Khera, women sang: "Everyone will come to your home, your family and neighbors, and ask to see your happy baby. Everyone will come with love."
Within 18 months, the approach had lowered infant mortality in the villages by half. "Saving the lives of newborns became the goal of the community," Kumar says. "Reducing infant mortality was a way of coming together. It was empowering."
Saksham reversed the direction of conventional development thinking, which views the recipients of innovation or aid as the last link in a long chain. Kumar's group treated the communities as the first mile. That's where the work, particularly behavior change, should start, he says. "It has to be supported socially," he adds.
Once more newborns survived at birth, Kumar extended his behavior-change efforts to improve what mothers and children eat, and how they keep their environments clean, to lower the rates of stunted growth. His team monitors new pregnancies in the villages and gathers moms-to-be for nutrition education and hygiene awareness.
Saksham's success prompted new government programs that sent health workers into the communities and that provided a monetary incentive for women to give birth in hospitals or clinics. By 2012, as these campaigns spread across the country, India's under-five mortality rate had decreased by almost 40 percent. But this has strained the country's health infrastructure.
This stress is evident at the Shivgarh hospital, a hulking facility that can barely contain the demand. A small ambulance fleet is overwhelmed; pregnant women arrive on wagons pulled by bicycle rickshaw drivers or on the backs of motorcycles. Inside, wheelchairs and gurneys are scarce. The delivery room has just two beds. Babies are sometimes born in the hallway, the bathroom, or outside the hospital. The four beds in the maternity ward afford only a brief respite; new moms often head back home – again on rickshaw wagons or motorcycles – after an hour or two of recovery.
So Kumar is turning from the communities to the facilities, to make them partners in behavior change by improving services for newborns. During the first phase of Saksham, he says, "90 percent of the births were at home and 10 percent in facilities. Now it's reversed. This is the opportunity to embed this behavior change, to have the facilities become centers of information."
He again holds up his hand. "You don't just want to know that these five essentials of newborn care, of behavior change, are important, but why. Then you get motivation. The mothers think, 'I want to improve. I want our children to survive and do well.'


