Story
 July 24, 2019
July 24, 2019
Science Under Fire: Ebola Researchers Fight to Test Drugs and Vaccines in a War Zone
Country:



Project
The Ebola Outbreak in North Kivu
What happens when Ebola hits in a war zone?

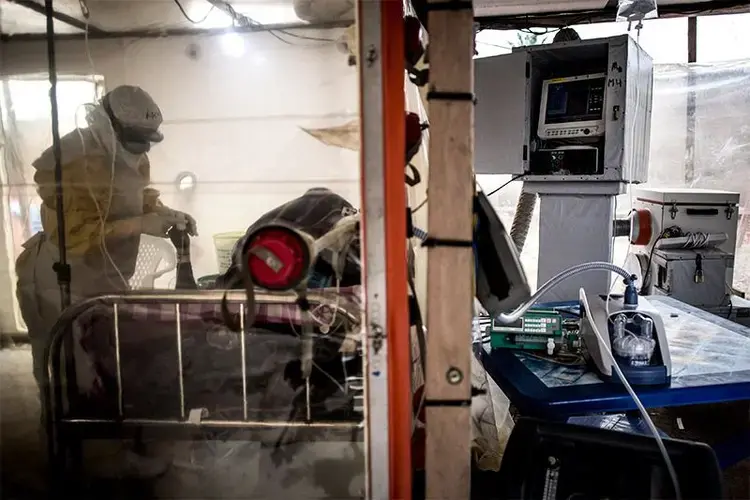
Heart and biochemistry monitors blink beside a woman curled up on a camp bed in an Ebola treatment centre. Her bed is encased in a transparent plastic cube to contain the virus, and an experimental drug flows through her veins.
The race to develop treatments for Ebola has accelerated since the largest epidemic in history devastated West Africa between 2014 and 2016. Scientists responding to the ongoing outbreak in the Democratic Republic of the Congo (DRC) have enrolled more than 500 participants in an unprecedented study of experimental drugs, vaccinated nearly 170,000 people, and sequenced the genomes of more than 270 Ebola samples collected from the sick.
“This outbreak is clearly a milestone for rigorous, good research,” says David Heymann, an epidemiologist at the London School of Hygiene and Tropical Medicine. “We will get definitive answers.”
Progress is sorely needed. The year-old DRC outbreak is the second largest on record and the first to strike in a war zone. Violence has hampered efforts to contain the virus, prompting the World Health Organization (WHO) to declare a ‘public health emergency of international concern’ on 17 July. The agency says that nearly 2,600 people in the DRC have been infected with Ebola and more than 1,700 have died.
Working in a conflict zone has forced researchers to adapt and persevere to an extraordinary degree. They have learned how to conduct rigorous studies in areas where killings, abductions and arson are commonplace, and where Ebola responders have come under repeated attack. Although biomedical advances alone cannot defeat Ebola, scientists studying this outbreak remain hopeful that their growing knowledge will help end it — and limit those to come.
“It is not easy,” says Jean Jacques Muyembe Tamfum, a microbiologist who helped to discover Ebola and now directs the National Institute for Biomedical Research (INRB) in Kinshasa. “You are doing this and people are shooting.”
He and other Congolese researchers are also working to ensure that any advances will benefit their homeland, which has experienced more Ebola outbreaks than any other. “It is very important to have the research done here because at the end of the day, Ebola is our problem,” says Sabue Mulangu, an infectious-disease researcher at the INRB.
Desperate Measures
Muyembe first encountered Ebola in 1976, while investigating a spate of deaths in Yambuku, a village in the northern DRC. As he collected blood from the sick, he noticed that their wounds did not clot. “My fingers were covered in blood,” he says. The samples were shipped to laboratories in Antwerp, Belgium, and Atlanta, Georgia, where virologists isolated Ebola and named it after the river that feeds Yambuku.
Scientists knew little about the virus until 1995, when an outbreak in Kikwit, DRC, killed 245 people in six months. Muyembe, Heymann and other researchers documented how the virus causes a person to haemorrhage internally until their organs fail. Desperate for a cure, Muyembe transfused blood from people who had beaten Ebola — which he suspected was rich with antibodies against the virus — into eight people in the throes of the disease. Seven survived.
Subsequent studies in monkeys at the US National Institute of Allergies and Infectious Diseases (NIAID) in Bethesda, Maryland, failed to replicate the result, but Muyembe refused to give up. “In my mind I was saying there should be a truth in here,” he recalls in his office in Kinshasa. A poster featuring portraits of four nuns who died in Kikwit hangs on one wall.
In 2006, Muyembe sent two Kikwit survivors to NIAID, where researchers — including Mulangu — isolated and studied the volunteers’ antibodies. One of the drugs being tested in the latest outbreak, mAb114, is based on antibodies from these Kikwit survivors.
The medicine was one of several that the DRC government approved for compassionate use shortly before the outbreak was declared in August 2018. Also included were two other antibody treatments — ZMapp and REGN–EB3 — and an antiviral drug, remdesivir.
But researchers pushed for a clinical trial to determine which therapy worked best. “It would be frustrating to use these interventions, but at the end of the outbreak have no more knowledge than when you started,” says Anthony Fauci, the director of NIAID.
He and other scientists ultimately drew up a blueprint for a randomized clinical trial that compares the four drugs, ensuring that every person who participates receives one of the treatments. Their innovative design allows the trial to stop and start as needed. That flexibility has proven crucial amid the ever-present violence in the Grand Nord region, where Ebola is spreading.
' People Want To Kill Me '
Every aspect of the outbreak is affected by the area’s long history of conflict and trauma. Residents have endured more than two decades of terror from armed groups, along with resource exploitation, political instability and neglect from the world at large. That has bred distrust of authorities — including foreign health workers — and conspiracy theories about why Ebola is thriving. One popular rumour alleges that Ebola responders inject people with deadly substances at treatment centres and vaccination sites.
These false ideas have fostered nearly 200 attacks on Ebola responders and treatment centres so far this year, according to the WHO. Seven people have been killed and 58 injured.

To adapt to the conflict, clinical researchers at an Ebola centre in Beni operated by the French medical charity ALIMA give mobile phones to patients who check out of the clinic. This allows them to stay in touch about lingering symptoms, even if violence makes it impossible to keep follow-up appointments. Many people use the service as an emergency helpline, says Émilie Gaudin, a support officer at ALIMA. “Sometimes a patient calls us and says, ‘People want to kill me,’ or ‘I want to kill myself.’”
Despite this difficult environment, the drug trial is nearing completion. Researchers are 14 people shy of their goal of enrolling 545 participants, a threshold that should allow them to draw strong conclusions about the drugs’ efficacy. But there are already hints that the treatments are working. The mortality rate at Ebola treatment centres, where all patients receive one of the experimental drugs, is 35–40% — compared with 67% overall in this outbreak. The latter figure reflects the large number of people who have died at home or in facilities that aren’t equipped to treat Ebola.
Violence has also hampered vaccination efforts. A few months ago, Diallo Abdourahamane, the WHO’s Ebola vaccine coordinator, heard about a man in the town of Katwa who his team had immunized with an experimental Ebola vaccine made by the pharmaceutical company Merck. The man had told sceptical onlookers that the vaccine would protect against the disease. “But after the team left,” Abdourahamane says, “the neighbours came and surrounded him at night. They said ‘You are the one helping to bring Ebola to our area’ — and they killed him.”
That traumatic experience prompted Abdourahamane and his colleagues to change how they vaccinate people. Their original strategy, which Abdourahamane had used with the same vaccine in Guinea in 2016, involved setting up a vaccination site close to the homes of a sick person’s contacts, and offering them the injection. Now, they give contacts the option to be vaccinated in neighbouring towns, away from prying eyes. Borrowing a term from the short-term sales spaces known as pop-up shops, they call this ‘pop-up vaccination’.
The team has also developed a strategy for vaccinating people when violence makes it too risky to track contacts. This evolved when Ebola began to spread among the Mai-Mai, militia groups in the eastern DRC. “If they accept vaccination, they usually don’t want us to come in with security,” meaning troops and police officers, Abdourahamane says. “So we come without security, but we don’t want to stay for long.”
But attacks against Ebola responders have thwarted plans to sequence Ebola virus genomes in Katwa. An Ebola treatment centre there was set ablaze in February and shot at in March, and in April a WHO epidemiologist was killed in the nearby city of Butembo. For now, researchers at the INRB have decided to continue shipping most blood samples from Ebola patients across the country to Kinshasa for genomic analysis.
Building Knowledge
Mosquitoes swarm the INRB campus at dusk in mid-June and goats graze on the lawn. It’s the first time all day that microbiologist Steve Ahuka has taken a break. He and his colleagues have been inundated with work since the outbreak began, and they’ve had to prioritize the research that could have the greatest immediate impact.

The scientists’ first genetic analyses of Ebola virus samples confirmed that the Merck vaccine, rVSV-ZEBOV, would elicit an effective immune response. Now they are rushing to sequence virus samples collected from areas where Ebola has just reached — including Uganda, where three people were diagnosed in June. By comparing that data with the genetic make-up of Ebola samples collected elsewhere, they can determine where people were infected. Ebola responders use this information to track down others who might have been exposed to the virus.
When the outbreak finally ends, Ahuka says his colleagues will have time to publish their work and post the genomic sequences online. They also hope to explore questions that they have not had time to address so far, such as whether certain Ebola mutations are associated with a higher risk of death.
The INRB is using money from the Japanese government to build a biobank to store blood samples that contain Ebola. When it’s complete, researchers from outside the DRC will be able to apply to study the samples in Kinshasa — but the DRC government won’t send the specimens out of the country. “We would like to avoid what happened in western Africa,” says Ahuka, who worked at a molecular-biology lab in Guinea during the 2014–16 outbreak. “We handled many samples and assumed they belonged to the country,” he remembers. “But all the samples were shipped out.”
In the end, many of the scientific papers and patents based on blood samples collected during the West Africa outbreak were authored by scientists at institutions in the United States and Europe. This frustrated researchers in the countries ravaged by the virus, who had hoped that studying aspects of the epidemic would strengthen their ability to respond to future infectious-disease outbreaks.
Heymann, who collaborated with Muyembe during the Kikwit outbreak 25 years ago, understands Congolese researchers’ position. “We should want them to have the capacity to do this themselves,” he says, “because they know their culture best.”
 in Katwa. Image by John Wessels. Democratic Republic of Congo, 2019.")
Education Resource
Meet the Journalist: Amy Maxmen
The Democratic Republic of the Congo experienced the second largest Ebola outbreak in history. But...




